IVF Questions
IVF treatment is complex and couples often have numerous questions about aspects of their treatment. Here we tackle some of the commonly asked questions.
How should I choose a clinic?
Fertility treatment is often complex. Highly skilled professionals, including fertility doctors, embryologists and fertility nurses will look after you during your treatment. It is really important that you have confidence in the clinical team. Some key information to look for when choosing your clinic:
- Who are the doctors, embryologists and nurses in that clinic? What is there background and experience? You will want an experienced team with track-record.
- What are the pregnancy success rates for various types of treatments? When comparing success rates, it is very important to compare ‘like with like’, that is, what is success rate for a comparable patient group (for instance, women under 35 years of age having the first cycle of IVF treatment).
- What is the range of services provided in the clinic? Does it include advanced tests and treatments?
- What is the waiting time for treatment?
- What are the costs of treatment? Is it ‘all-inclusive price’? This is important to avoid nasty surprises!
- What is the feel of the clinic? If it feels rushed and impersonal, avoid it!
The choice of IVF clinic is a key decision. You should make a decision only after visiting a clinic and only after speaking with some staff in the clinic.
How successful is IVF?
The success very much depends on your age, fertility history and test results.
Overall Human Fertility and Embryology Authority Success Rates across the country are:
-
-
- 29% for women under 35
- 23% for women aged 35 to 37
- 15% for women aged 38 to 39
- 9% for women aged 40 to 42
- 3% for women aged 43 to 44
- 2% for women aged over 44
-
Overall Human Fertility and Embryology Authority Success Rates across the country are:
- 29% for women under 35
- 23% for women aged 35 to 37
- 15% for women aged 38 to 39
- 9% for women aged 40 to 42
- 3% for women aged 43 to 44
- 2% for women aged over 44
You can find out average success rates for various clinics by visiting the human fertilisation and embryology authority (HFEA) website.
Typical fertility treatment results for
CARE Fertility Birmingham Clinic.
September 2017 – February 2018:
Implantation rate was 45% for fresh IVF/ICSI cycles for women under 38 years of age (with own eggs).
Clinical pregnancy rate was 43% per cycle started for fresh IVF/ICSI cycles for women under 38 years of age.
Typical fertility treatment results for
CARE Fertility Birmingham Clinic:ars of age.
September 2017 – February 2018:
Implantation rate was 45% for fresh IVF/ICSI cycles for women under 38 years of age (with own eggs).
Clinical pregnancy rate was 43% per cycle started for fresh IVF/ICSI cycles for women under 38 years of age.
What happens to the eggs and embryos not used during IVF treatment?
Conventional IVF treatment involves retrieval of multiple eggs which are then mixed with sperm, to create embryos. The best one or two embryos are transferred to provide the best chance of a pregnancy. The surplus embryos can be frozen and kept for your future use, can be donated for research (with your full consent) or be allowed to perish if the quality of the embryos would not allow storage.
Am I too old for IVF?
In general, the result of your IVF treatment is dependent on your age. However, some women have a good store of eggs at older ages, whilst other women are unfortunate to have a low store of eggs in their ovaries even at young ages. The only way to find out whether you can have IVF treatment is to go and visit an IVF doctor for tests to assess your ovarian egg store. We can scan your ovaries and also take a few simple blood tests to be able to have an estimate of your egg store and how you might fare if you have IVF treatment.

Am I too old for IVF?
In general, the result of your IVF treatment is dependent on your age. However, some women have a good store of eggs at older ages, whilst other women are unfortunate to have a low store of eggs in their ovaries even at young ages. The only way to find out whether you can have IVF treatment is to go and visit an IVF doctor for tests to assess your ovarian egg store. We can scan your ovaries and also take a few simple blood tests to be able to have an estimate of your egg store and how you might fare if you have IVF treatment.
What are the side-effects of IVF?
Side effects are quite common for women who are having IVF treatment. Whilst you are taking the injections to gain control of your menstrual cycle, you can experience headaches, mood swings, abdominal bloating and hot flushes.
After egg collection, you may also have further bloating and some spotting of blood from the vagina. While you are taking progesterone to help support the lining of the womb and the pregnancy, you may experience breast tenderness, constipation and headaches too.
IVF treatment can also be linked to a serious complication called Ovarian Hyperstimulation Syndrome (sometimes referred to as OHSS). This is when the ovaries have been over-stimulated and start producing substances that can make you feel poorly. Symptoms include swelling of your abdomen, shortness of breath and not passing much urine. If you experience these symptoms, or feel unwell generally during your IVF treatment, you need to speak to your fertility doctor.
How many IVF cycles will I realistically need?
Some women are very lucky when it comes to their IVF treatment, getting pregnant after just one cycle of IVF. But many couples need more than one IVF treatment cycle to have a baby. A reasonable number of IVF cycles to consider when you start your fertility journey is 3. NICE, which is the UK’s professional body that produces practice guidelines, recommends that you could have three cycles of IVF, although many areas in the UK will only provide NHS funding for one cycle.
It is important to remember the overall success rates for IVF treatment is mainly dependent on age, so for example if you are over 40 you may need more IVF treatment cycles compared to someone who is under 35.

How much does an IVF treatment cycle cost? Are there really any ‘money back’ guarantee IVF funding packages?
IVF treatment costs vary widely between clinics. Some clinics charge an ‘all-inclusive’ fee, and others charge a low ‘base-line’ fee, but then surprise you with unexpected additional costs! It is very important to understand exactly what you will be getting for the fees that you pay. A good clinic will give you all the details that you need to help you make a sound decision. An average ‘all-inclusive’ fee for IVF treatment is about £3500. The cost of medicines will need to be added to this.
Some clinics that are confident with their clinical care and success rates offer a ‘money back’ guarantee, that is, if you don’t have a baby at the end of your treatment programme, you will be given your money back! Here are details of a money-back guarantee IVF programme at CARE Fertility Birmingham.
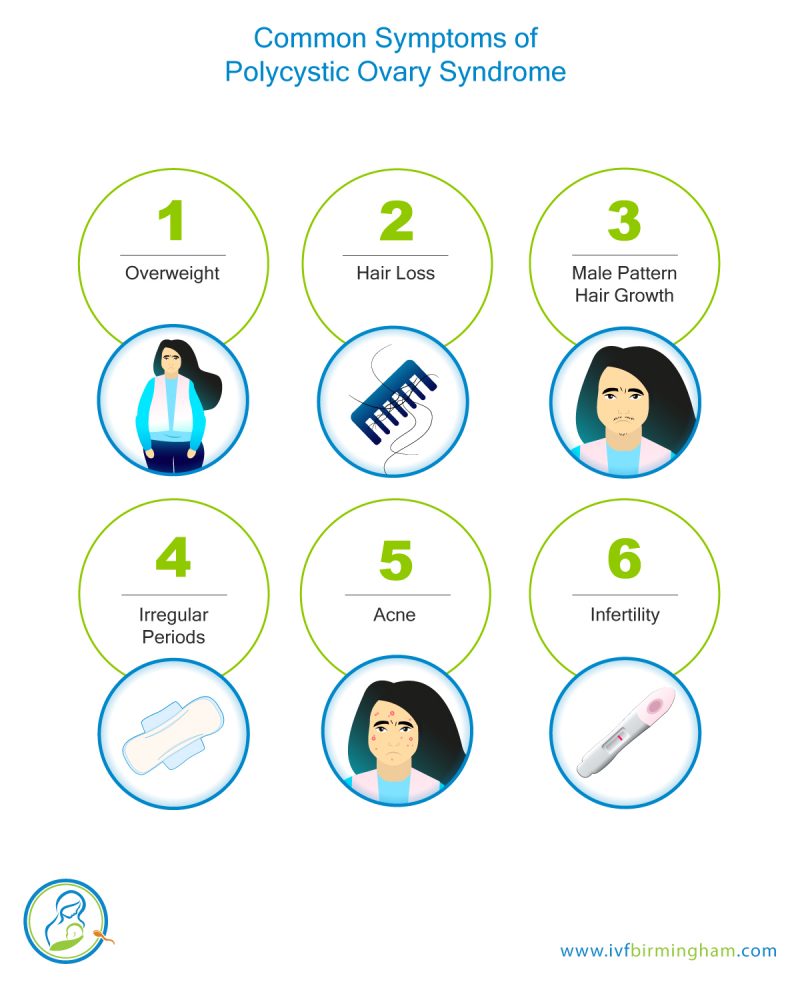
I have polycystic ovary syndrome (PCOS). What is the impact of this on fertility and IVF? What can I do?
You may have been diagnosed with PCOS because of infrequent or absent menstrual bleeds, symptoms such as acne, excessing hair growth or weight gain, presence of too many follicles on pelvic ultrasound scan (‘polycystic ovaries’) or higher than expected levels of male-type hormones in your blood test.
Many women with PCOS do not ovulate (releasing eggs from their ovaries). Sometimes, losing weight is all that is required for you to start to ovulate. If losing weight alone is not enough, then there are several medicines (including clomiphene, letrozole, metformin and FSH injection) that can help achieve ovulation. A key-hole operation called ‘ovarian diathermy’ may be suitable for some women. Many women with PCOS, however, will need IVF to help them achieve a pregnancy.
Women with PCOS having IVF may produce a large number of eggs, but many of these eggs could be of poor quality. Another potential problem is the development of a serious condition called the ovarian hyperstimulation syndrome (OHSS). With OHSS, fluid can accumulate in the abdomen, around the chest and sometimes even around the heart; clots can develop in the legs, chest or other parts of the body. Patients with OHSS can become very unwell. So, IVF clinics take special care to do all they can to reduce the risk of OHSS developing.
The first step in preparing for IVF is to ensure your body weight is as best as it can be. You can find some advice on this in our previous question. You may be started on a course of metformin to reduce the risk of OHSS; metformin is often started about a month before your IVF cycle. You are likely to have a ‘short antagonist protocol’ and a gentle ovarian stimulation with a low dose FSH injections. You will have ultrasounds, and often oestradiol blood tests, to monitor the progress of follicular (egg sac) development. If too many follicles develop, you may have your FSH injection dose reduced, or altogether omitted for a few days. Omitting FSH injections is called ‘coasting’. The final egg maturation (‘trigger’) injection may be with an ‘agonist trigger’ rather than the usual HCG injection; we will guide you on all of these steps, so don’t worry about trying to remember it all. You may also be given a course of cabergoline tablets to reduce the risk of OHSS.
If there is significant risk of OHSS, we may suggest not going ahead with a fresh embryo transfer, but instead freezing all the embryos for a transfer a month or two later. During and after IVF treatment, we will ask you to look out for OHSS symptoms, such as bloating and abdominal distension, nausea and vomiting, breathing difficulty, not passing much urine and leg pain.
I have repeated unsuccessful IVF treatment cycles. What can I do?
There may be a number of reasons why you may have repeated unsuccessful attempts at IVF treatment. The most common reason would be age related. As women age, their store of eggs reduce in both quantity and quality. A reduction in quantity of eggs will mean that the embryology team have fewer embryos to choose from to select the best one. A reduction in quality will lead to poorer quality embryos, which are less likely to cause a pregnancy and more likely to lead to miscarriage.
In some women, there are no concerns regarding egg number or quality and despite the transfer of high quality embryos, these women can still get negative pregnancy tests or miscarry. This condition is called recurrent implantation dysfunction and can be caused by a number of factors, including the inability of the lining of the womb to allow pregnancy (endometrial receptivity), problems with the womb (such as a fibroid, septum or polyp), sticky blood disorders, hormonal imbalances or problems with the immune system.
There are numerous tests and treatments that are available for recurrent implantation dysfunction {link}. However, you and your doctor will need to look at the evidence for these tests and treatments carefully before deciding to move forward with them.
I have repeated unsuccessful IVF treatment cycles. What can I do?
There may be a number of reasons why you may have repeated unsuccessful attempts at IVF treatment. The most common reason would be age related. As women age, their store of eggs reduce in both quantity and quality. A reduction in quantity of eggs will mean that the embryology team have fewer embryos to choose from to select the best one. A reduction in quality will lead to poorer quality embryos, which are less likely to cause a pregnancy and more likely to lead to miscarriage.
In some women, there are no concerns regarding egg number or quality and despite the transfer of high quality embryos, these women can still get negative pregnancy tests or miscarry. This condition is called recurrent implantation dysfunction and can be caused by a number of factors, including the inability of the lining of the womb to allow pregnancy (endometrial receptivity), problems with the womb (such as a fibroid, septum or polyp), sticky blood disorders, hormonal imbalances or problems with the immune system.
There are numerous tests and treatments that are available for recurrent implantation dysfunction {link}. However, you and your doctor will need to look at the evidence for these tests and treatments carefully before deciding to move forward with them.
I have a low AMH. What are my prospects with IVF?
Anti-Mullerian hormone, or AMH, is rapidly establishing itself as the centre-piece of fertility investigations. It is a blood test, and it can be done at any time in a menstrual cycle.
Here is a general guide to interpreting AMH results:
- If the AMH result is <1pmol/l, this means the egg store is extremely low, and natural or IVF pregnancy chances are extremely poor. Your doctor may suggest that you should consider donor egg treatment.
- If the AMH result is between 1-5 pmol/l, this means egg store is low. Treatment with your own eggs is possible, but there is a risk of cancellation of an IVF cycle if no eggs are obtained.
- If the AMH is between 5-14 pmol/l, this suggests a satisfactory store of eggs, and a good outcome can be expected from IVF treatment.
- If the AMH is between 14 – 30, this means a good store of eggs, and the prospects for good outcome from IVF are excellent.
- AMH >30 pmol/l indicates a high store of eggs. On the face of it, this may seem a good thing, but patients with high AMH are at risk of ovarian hyperstimulation syndrome, or OHSS, which can be a serious condition. Very high AMH is therefore not ideal. Having said that, they are many steps that we can take to reduce the risk of OHSS, and your doctors and nurses will take special care to minimise the risks associated with OHSS.

If your AMH is not normal, we would advise a consultation with a fertility specialist. Your specialist will not interpret the AMH result in isolation, but will also look at your age, clinical history, and the results of other egg store tests. The fertility specialist will then be able to give you the percentage chances of pregnancy with IVF using your own eggs versus donor eggs. The percentage chance of pregnancy will vary from clinic to clinic, so it is not possible to give a single simple answer, but your fertility clinic should be able to help.
I have high BMI (overweight). What is the impact of that on fertility and IVF? What can I do?
A high body mass index (BMI) is unfortunately linked to reduced fertility in women and men. A woman with a high BMI often needs larger doses of IVF medications, and may have poor development of ovarian follicles (which are sacs containing the eggs), poor quality eggs, poor endometrium (lining of the womb) and a higher risk of miscarriage and other pregnancy complications. So, it really helps if you are able to lose weight before you have fertility treatment. The ideal is if you are able to get below a BMI of 30. If this is not possible, it would be better if you are able to get below a BMI of 35, which is the cut-off for offering treatment at CARE Fertility Birmingham Clinic. You can find out your BMI by entering your height and weight on to a BMI calculator; just search ‘BMI calculator’ on Google.
Some patients may benefit from medicines such as orlistat or sibutramine, or bariatric surgery. You may want to discuss these with your doctor, but even such medical treatment can only help if you are already losing weight through exercise and healthy eating.
We find patients who lose weight often have 4 successful elements to their approach:
- They set reasonable weight targets (rather than unrealistic ones which are difficult to achieve), and keep a record of their progress on a diary.
- They eat healthy AND exercise (rather than doing one or the other). Note we said ‘healthy eating’ rather than ‘dieting’! Yes, you may need to control the calories you consume (dieting), but healthy eating in the form of reducing meat (that includes chicken!), fats and sugar and increasing fruits and vegetable should be the first step.
- They often take part in a group program, which keeps them motivated. You and your partner can form a group! Or you can find a group near you on Google.
- They practise ‘stimulus control’ which is a fancy term for not keeping the wrong sort of food visible in your kitchen! For example, this may mean swapping the tin of biscuits on your dining table with a bowl of fruits.
I have high BMI (overweight). What is the impact of that on fertility and IVF? What can I do?
A high body mass index (BMI) is unfortunately linked to reduced fertility in women and men. A woman with a high BMI often needs larger doses of IVF medications, and may have poor development of ovarian follicles (which are sacs containing the eggs), poor quality eggs, poor endometrium (lining of the womb) and a higher risk of miscarriage and other pregnancy complications. So, it really helps if you are able to lose weight before you have fertility treatment. The ideal is if you are able to get below a BMI of 30. If this is not possible, it would be better if you are able to get below a BMI of 35, which is the cut-off for offering treatment at CARE Fertility Birmingham Clinic. You can find out your BMI by entering your height and weight on to a BMI calculator; just search ‘BMI calculator’ on Google.
Some patients may benefit from medicines such as orlistat or sibutramine, or bariatric surgery. You may want to discuss these with your doctor, but even such medical treatment can only help if you are already losing weight through exercise and healthy eating.
We find patients who lose weight often have 4 successful elements to their approach:
- They set reasonable weight targets (rather than unrealistic ones which are difficult to achieve), and keep a record of their progress on a diary.
- They eat healthy AND exercise (rather than doing one or the other). Note we said ‘healthy eating’ rather than ‘dieting’! Yes, you may need to control the calories you consume (dieting), but healthy eating in the form of reducing meat (that includes chicken!), fats and sugar and increasing fruits and vegetable should be the first step.
- They often take part in a group program, which keeps them motivated. You and your partner can form a group! Or you can find a group near you on Google.
- They practise ‘stimulus control’ which is a fancy term for not keeping the wrong sort of food visible in your kitchen! For example, this may mean swapping the tin of biscuits on your dining table with a bowl of fruits.
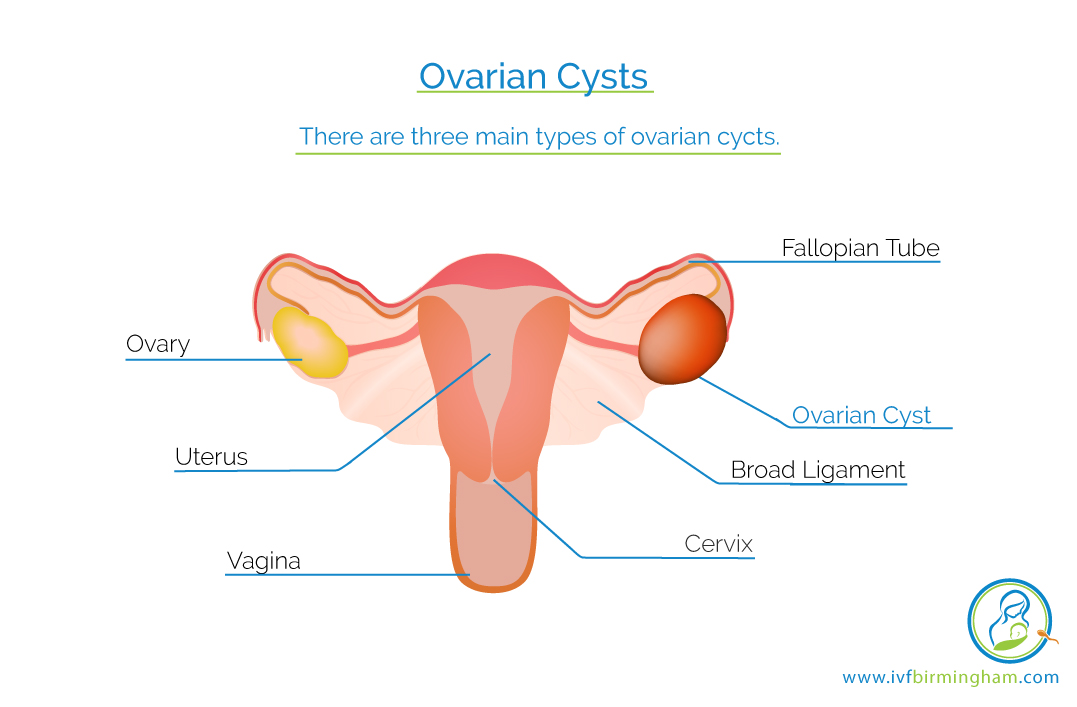
I have been diagnosed to have a cyst in the ovary. What is the impact of this on IVF?
The impact on IVF will depend on what type of ovarian cyst you have. There are at least three types of ovarian cysts: ‘simple’ cysts, which are thin walled and have fluid inside them without any solid contents, endometriotic cysts, and tumours (which can be benign, such a dermoid cyst or extremely rarely cancerous tumours).
Simple cysts can be ‘functional’ (which means they secrete the hormone oestrogen) or ‘non-functional’ (which means they do not secrete oestrogen). If it is a small simple cyst, they you can go ahead with IVF treatment. If it is a large simple cyst or one that is persisting over several months, then your doctor may advise some blood tests (tumour markers: CA125, AFP, HCG and LDH) and aspiration or removal of the cyst. There is some evidence that the presence of a simple cyst can be associated with a poor ovarian response to IVF medicines, but there is no evidence that aspirating or removing the cyst improves the outcomes. So, you will need to have a good discussion with your doctor about the best way forward.
If it is an endometriotic cyst, you may need to have it removed. Please see below.
If it is a tumour, then you will need a consultation with a gynaecologist. A small benign tumour, like a dermoid cyst, may not need anything being done to it. A larger cyst or one that has a cancerous appearance will require an urgent medical consultation.
Finally, there are women who tend to develop ovarian cysts time after time. In such a situation, using contraceptive pill before starting IVF and using an ‘antagonist’ protocol may be of helpful.
I have been diagnosed to have a cyst in the ovary. What is the impact of this on IVF?
The impact on IVF will depend on what type of ovarian cyst you have. There are at least three types of ovarian cysts: ‘simple’ cysts, which are thin walled and have fluid inside them without any solid contents, endometriotic cysts, and tumours (which can be benign, such a dermoid cyst or extremely rarely cancerous tumours).
Simple cysts can be ‘functional’ (which means they secrete the hormone oestrogen) or ‘non-functional’ (which means they do not secrete oestrogen). If it is a small simple cyst, they you can go ahead with IVF treatment. If it is a large simple cyst or one that is persisting over several months, then your doctor may advise some blood tests (tumour markers: CA125, AFP, HCG and LDH) and aspiration or removal of the cyst. There is some evidence that the presence of a simple cyst can be associated with a poor ovarian response to IVF medicines, but there is no evidence that aspirating or removing the cyst improves the outcomes. So, you will need to have a good discussion with your doctor about the best way forward.
If it is an endometriotic cyst, you may need to have it removed. Please see below.
If it is a tumour, then you will need a consultation with a gynaecologist. A small benign tumour, like a dermoid cyst, may not need anything being done to it. A larger cyst or one that has a cancerous appearance will require an urgent medical consultation.
Finally, there are women who tend to develop ovarian cysts time after time. In such a situation, using contraceptive pill before starting IVF and using an ‘antagonist’ protocol may be of helpful.
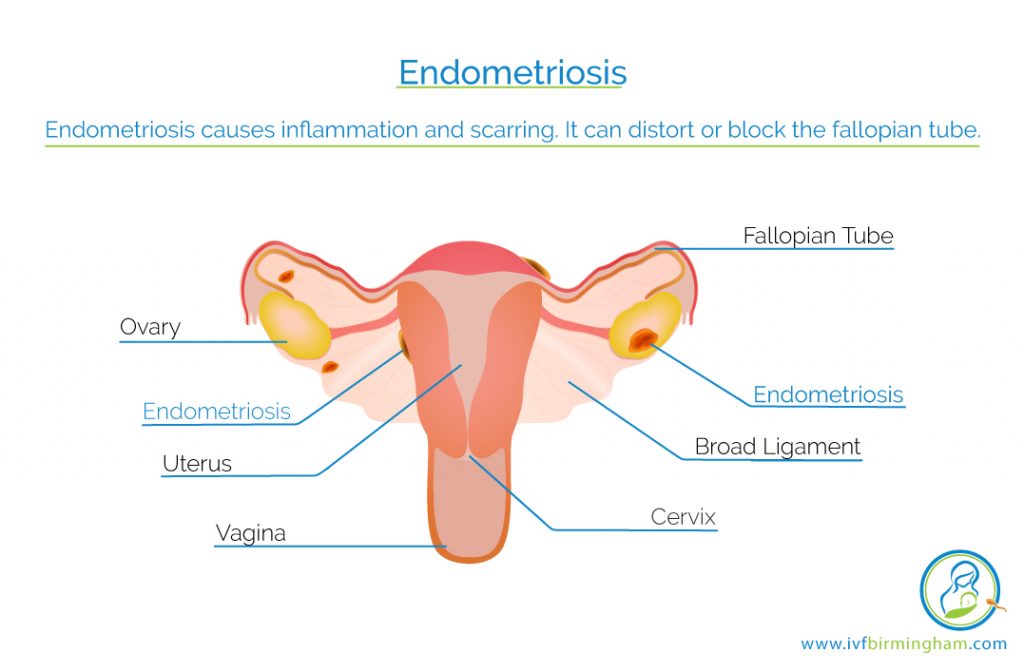
I have endometriosis. What is the impact of this on fertility and IVF outcome?
Endometriosis can be found in the pelvis, or it can also implant inside the ovary and cause an ovarian cyst – this is called an endometrioma. Endometriosis causes inflammation and scarring. It can distort or block the fallopian tube.
Research evidence shows endometriosis reduces your fertility chances. We carried out a comprehensive analysis of the data a few years ago. We found that endometriosis was associated with reduction in fertilization, implantation and pregnancy rates. If you have endometriosis in the ovary, that may mean we gather fewer eggs during IVF treatment.
How can we treat endometriosis? There is still much debate about how to treat endometriosis to improve fertility outcomes. The treatment will depend on the extent of the disease, and the clinical history. If the endometriosis is mild, then surgery to remove the endometriosis is an option. It can improve natural pregnancy chances. If that does not work, most doctors will advise IUI, or intrauterine insemination, combined with ovarian stimulation. Couples usually have 3 to 4 cycles of IUI treatment. If that does not work, then IVF treatment is often recommended.
If a patient has moderate or severe endometriosis, then it may be reasonable to go straight to IVF treatment. There is some interesting data suggesting pre-treatment with a medicine called GnRH analogues for 3-6 months before IVF can improve the pregnancy chances.
If a patient has an endometrioma, that is an endometriotic cyst in the ovary, what we do depends on the size of the cyst. Generally, if the cyst is more than 4cm, many doctors will recommend removal of it through key-hole surgery, before proceeding with IVF. If the endometriotic cyst is less than 4 cm, patients can normally go ahead with IVF without needing surgery first. These are the treatment principles, but please seek a fertility consultation to understand what may be the right course of action for you.
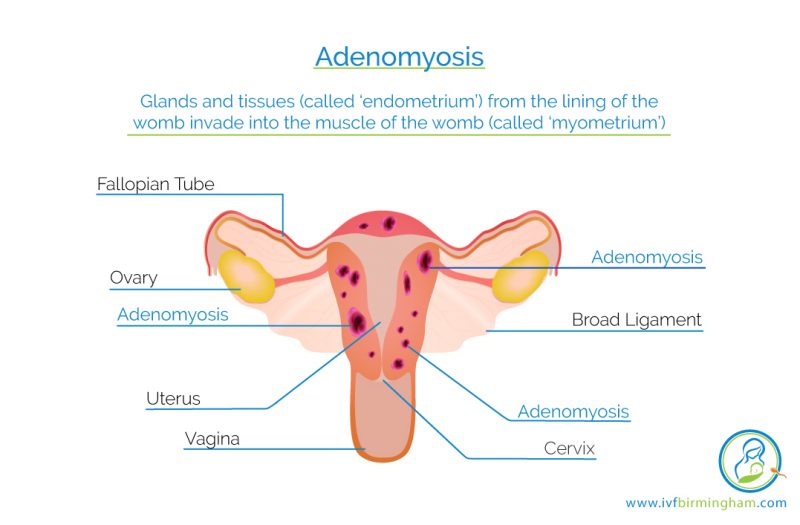
I have adenomyosis. I am due to have IVF. What is the right course of action for me?
Adenomyosis is when the glands and the tissues (called the ‘endometrium’) from the lining of the womb invade into the muscle of the womb (called the ‘myometrium’). Symptoms include painful and heavy menstrual periods. Adenomyosis is diagnosed on ultrasound scan, or occasionally on MRI scan. It is linked to a 28% reduction in pregnancy rates and doubling in the risk of miscarriage rates after IVF treatment. The difficulty is that we have limited evidence on how we can manage patients with adenomyosis. It appears a long GnRH analogue protocol may be better than a short protocol. If a long protocol with fresh embryo transfer does not work, then it may be helpful to consider freezing all embryos in a future IVF cycle, then having 3 months of treatment with GnRH analogue, and then having a frozen embryo transfer. It is well worth having a detailed discussion with a fertility specialist if you have a diagnosis of adenomyosis.
I have fibroids. What does this mean to my fertility and IVF treatment?
They are benign growths made up of uterine muscle and fibrous tissues. They are very common, but many women don’t know that they have fibroids as they don’t always cause symptoms. But in some women, they can cause heavy periods, painful periods, constipation, backpain, and discomfort during sex. They can also be linked to infertility and miscarriage. They can affect the movement of the sperm and embryo, disturb the blood flow to the lining of the womb, and compromise implantation.
It is important to appreciate that not all fibroids are the same. Whether they have an impact on fertility or not and whether they need removal or not depends on, firstly, the location of fibroids, secondly number of the fibroids, and thirdly the size of the fibroids. You will need to have a clinical consultation to determine the right course of action for you. Here we provide some general advice.
Fibroids are categorised into three groups depending on where they are in the uterus. First, and the most problematic ones, are the submucous fibroids. They sit near the womb lining, and distort the womb cavity, and increase the risks of infertility and miscarriage. A meta-analysis, which is a synthesis of many studies, showed submucous fibroids were associated with a 72% reduction in implantation, 64% reduction in pregnancy rates, and a 68% increase in miscarriage rates.
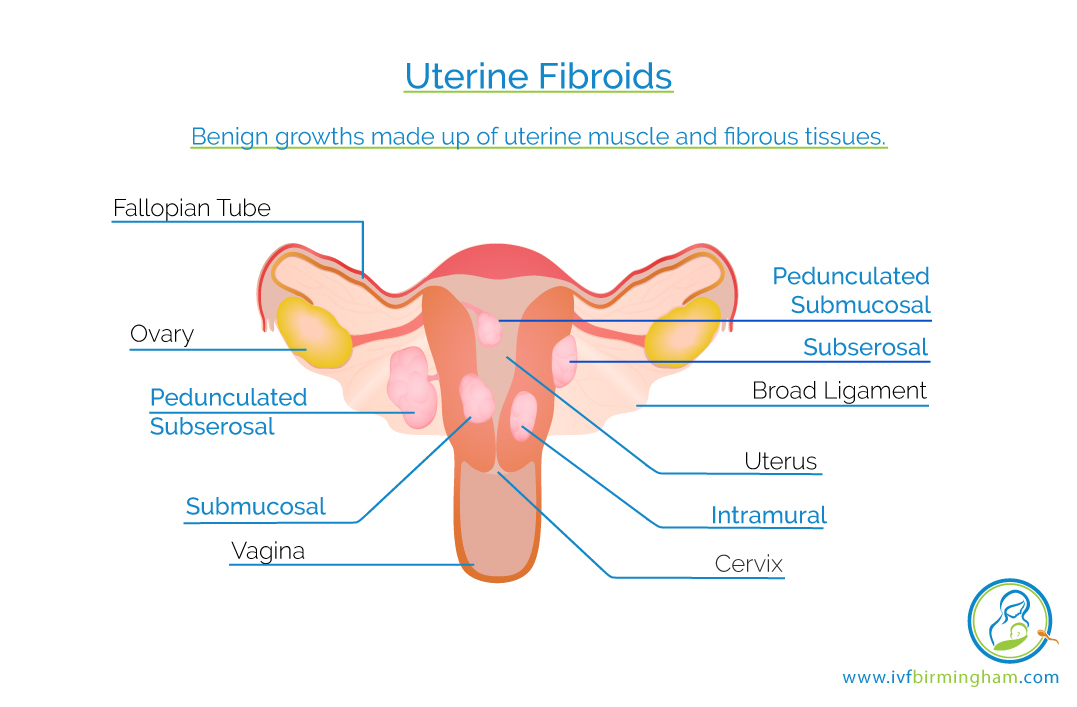
They sit near the womb lining, and distort the womb cavity, and increase the risks of infertility and miscarriage. A meta-analysis, which is a synthesis of many studies, showed submucous fibroids were associated with a 72% reduction in implantation, 64% reduction in pregnancy rates, and a 68% increase in miscarriage rates. So, it is not surprising that there is very little debate about whether they should be removed. Almost all clinicians would agree that they should be removed, and the good news is that the removal can be done through an operation through the vagina, without needing a cut on the abdomen.
The second type of fibroid is called intramural, and here the fibroids sit in the muscular wall of the uterus, but without distorting the womb cavity. The evidence of their association with poor fertility outcome is less clear-cut, but a study by our group did find a 15% reduction in pregnancy rate with this type of fibroids. However, we do not know if removing these fibroids will improve outcomes of fertility treatment – the evidence is simply not there. If removal is considered necessary, an operation called myomectomy will be needed. This is a major operation. It can be done via keyhole or open surgery. There are significant risks with this operation, including the risk of severe haemorrhage that may on occasions result in the catastrophic complication of removal of the uterus to control the bleeding and save the patient’s life. So, the decision for this operation should not be taken lightly. We would not normally recommend removal of intramural fibroids unless the fibroid is large, the patient has a history of repeated negative IVF cycles or miscarriages, or she has symptoms such as pain or heavy menstrual bleeding.
The third type of fibroid is called subserosal; the fibroids here develop outside the wall of the uterus. They do not have any impact on infertility or miscarriage, and do not generally need treatment.
Finally, a question that we get asked commonly these days: is there any way of treating fibroids without surgery? The answer is yes, and no! Yes, there are ways of reducing the volume of fibroids by using medicines such as GnRH analogue or by a technique called uterine artery embolization, but no, these approaches are not only unhelpful for patients who are having infertility treatment. Uterine artery embolization has been linked to premature failure of the ovaries and miscarriages. It is best to avoid uterine artery embolization if you are trying to have a baby.
Let us leave you with this final comforting thought: many women with fibroids don’t even know that they have them, and more often than not they have successful pregnancies without any medical intervention at all.
I have an endometrial polyp (polyp in the womb cavity). Would this affect my IVF chances?
Polyps are benign overgrowths in the lining of the womb. They are usually diagnosed on a pelvic ultrasound scan, often before a patient starts an IVF treatment, but occasionally only during the IVF treatment cycle. Polyps can be associated with failed implantation and miscarriage. So removal of polyps should be considered before starting an IVF treatment cycle. Polyp removal can be done through simple keyhole surgery, called ‘hysteroscopy’.
Polyps are benign overgrowths in the lining of the womb. They are usually diagnosed on a pelvic ultrasound scan, often before a patient starts an IVF treatment, but occasionally only during the IVF treatment cycle. Polyps can be associated with failed implantation and miscarriage. So removal of polyps should be considered before starting an IVF treatment cycle. Polyp removal can be done through simple keyhole surgery, called ‘hysteroscopy’
If a polyp is identified only during an IVF treatment cycle, the patient is left with the difficult decision about whether she should stop the IVF treatment and have the polyp removed, before proceeding with a new IVF cycle.
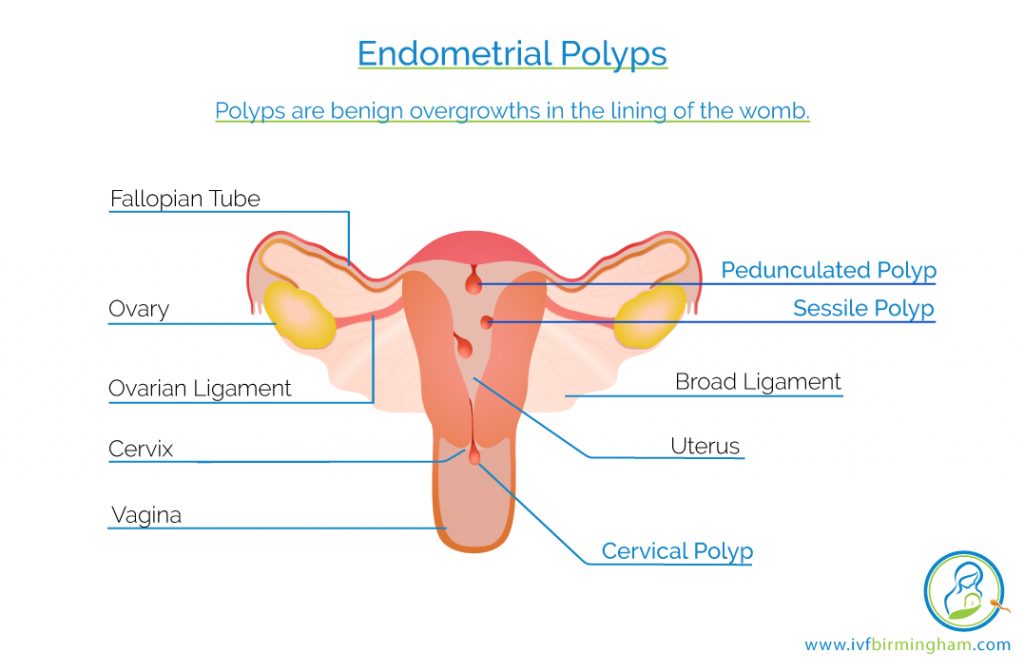
We normally advise that the IVF treatment does not need to be stopped if the polyp is small (less than 1.5 cm). If however, the polyp is large (more than 1.5 cm) or there are many polyps then we would advise the patient stopping the IVF treatment and having the polyp removed. There is also the option of proceeding with egg collection and freezing the embryos for future frozen transfer, 2 or 3 months after removal of the polyp(s). Your fertility consultant will advise you on the best cause of action.
I have an endometrial polyp (polyp in the womb cavity). Would this affect my IVF chances?
Polyps are benign overgrowths in the lining of the womb. They are usually diagnosed on a pelvic ultrasound scan, often before a patient starts an IVF treatment, but occasionally only during the IVF treatment cycle. Polyps can be associated with failed implantation and miscarriage. So removal of polyps should be considered before starting an IVF treatment cycle. Polyp removal can be done through simple keyhole surgery, called ‘hysteroscopy’.
Polyps are benign overgrowths in the lining of the womb. They are usually diagnosed on a pelvic ultrasound scan, often before a patient starts an IVF treatment, but occasionally only during the IVF treatment cycle. Polyps can be associated with failed implantation and miscarriage. So removal of polyps should be considered before starting an IVF treatment cycle. Polyp removal can be done through simple keyhole surgery, called ‘hysteroscopy’
If a polyp is identified only during an IVF treatment cycle, the patient is left with the difficult decision about whether she should stop the IVF treatment and have the polyp removed, before proceeding with a new IVF cycle.
We normally advise that the IVF treatment does not need to be stopped if the polyp is small (less than 1.5 cm). If however, the polyp is large (more than 1.5 cm) or there are many polyps then we would advise the patient stopping the IVF treatment and having the polyp removed. There is also the option of proceeding with egg collection and freezing the embryos for future frozen transfer, 2 or 3 months after removal of the polyp(s). Your fertility consultant will advise you on the best cause of action.
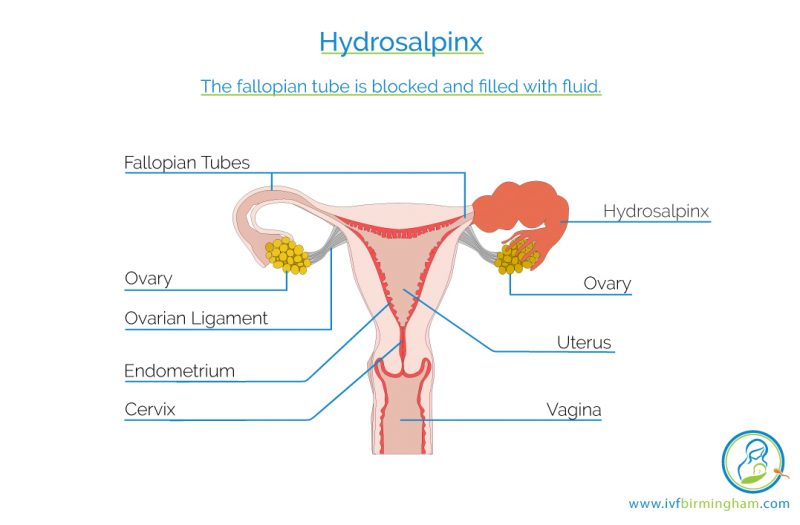
I have a hydrosalpinx (fluid filled blocked fallopian tube). What will be your advice?
Hydrosalpinx is when the fallopian tube is blocked and filled with fluid. Such a tube cannot allow the sperm and egg to meet when trying to conceive a natural pregnancy. The tube may have become blocked due to infection, endometriosis or previous surgery.
The advice that you will get from your IVF doctor will be depend on the nature of the swollen tube or tubes. If the swelling of the tubes is very severe, then you may be advised to have the tube or tubes removed or disconnected from the womb. This is because the fluid inside the tubes causing the swelling has been found to have a negative impact on your chances of getting pregnant from the IVF treatment.
If the tubes are mildly swollen then your IVF doctor may suggest a key-hole operation where an opening is made in the affected tube(s) to drain the fluid. You can then try for natural pregnancy or undergo IVF treatment. This tube conserving approach is better for those with milder disease and in younger women who have more time to try for pregnancy naturally.
I had a history of Chlamydia when I was young? What is the implication of this for my IVF treatment?
It is thought that as many as 1 in 10 people aged between 15 and 24 years are affected with chlamydia. It is the most common sexually transmitted infection in the UK.
Most women who are treated for chlamydia will have no problems getting pregnant naturally. However, in a small group of women, despite good treatment with antibiotics, chlamydia can cause infertility. Chlamydia infection can cause scarring or blockage of the fallopian tubes which may mean that the egg and sperm cannot meet to form a pregnancy when trying for a natural pregnancy. This may be the reason why you need IVF treatment. If you have had previous treatment of chlamydia, it is important to tell your IVF doctor as this may provide a clue as to why you are unable to get pregnant naturally.
If you have been treated for past chlamydia infection, your IVF treatment should be unaffected. However, your IVF doctor may test you for current chlamydia infection and you may need antibiotics before you begin your IVF treatment if the test is positive. In this situation, it is very important for you to complete the course of antibiotics.
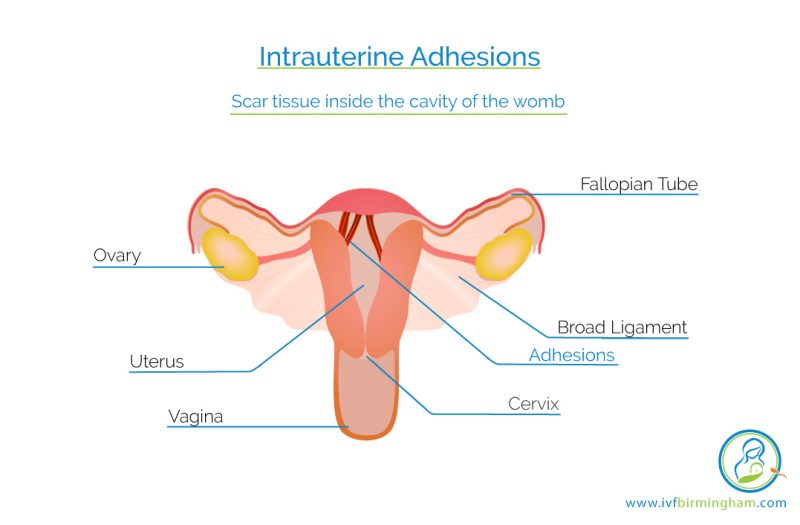
I have been told I have scar tissues (‘adhesions’) in the womb. What can be done?
Scar tissue inside the cavity of the womb can be caused by infections or previous surgery for termination of pregnancy or miscarriage. If you are found to have scar tissue inside the womb, your IVF doctor may suggest that you have a camera procedure inside your womb to remove it. This has been found to be of great benefit in some women preparing for IVF treatment.
I have been told I have scar tissues (‘adhesions’) in the womb. What can be done?
Scar tissue inside the cavity of the womb can be caused by infections or previous surgery for termination of pregnancy or miscarriage. If you are found to have scar tissue inside the womb, your IVF doctor may suggest that you have a camera procedure inside your womb to remove it. This has been found to be of great benefit in some women preparing for IVF treatment.
I have been told my womb lining (endometrium) does not develop well and I have a thin lining in fresh or frozen IVF cycles. What can be done?
The lining of the womb, known as endometrium, needs to be ‘receptive’ to an embryo for implantation and pregnancy occur. It is very well established that a very thin endometrium is associated with lower pregnancy and higher miscarriage rates. But what is ‘very thin’ endometrium? Most people will define this as less than or equal to 6mm. So, if you have a lining that is 7mm or more, then you are on safe grounds, although a lining between 10 – 15mm is ideal. It is important to note that it is not just the thickness of the womb lining that matters, but also its appearance. An appearance that we call ‘triple line’ is considered best.
So, what can be done? Unfortunately, there are no straight forward answers. If the lining is consistently thin, then it is important to assess the inside of the womb cavity with a keyhole camera (hysteroscopy) to see if a reason, for example scar tissues, could be seen. If the lining is thin during a fresh IVF cycle, then the option of freezing all the embryos should be considered. While the embryos are safely in the laboratory, we can try to thicken the womb lining in a frozen cycle, and if we achieve a good endometrial thickness, then we can thaw the embryos and transfer them. In a frozen cycle, high dose oestrogen tablets and patches can be used to thicken the lining. Some clinicians add medicines such as aspirin, steroids, pentoxifylline, tocopherol and Viagra to thicken the endometrium, but there is no clear evidence to support their use. Your IVF consultant would be able to advise the best way forward.
I have been told my womb lining (endometrium) does not develop well and I have a thin lining in fresh or frozen IVF cycles. What can be done?
The lining of the womb, known as endometrium, needs to be ‘receptive’ to an embryo for implantation and pregnancy occur. It is very well established that a very thin endometrium is associated with lower pregnancy and higher miscarriage rates. But what is ‘very thin’ endometrium? Most people will define this as less than or equal to 6mm. So, if you have a lining that is 7mm or more, then you are on safe grounds, although a lining between 10 – 15mm is ideal. It is important to note that it is not just the thickness of the womb lining that matters, but also its appearance. An appearance that we call ‘triple line’ is considered best.
So, what can be done? Unfortunately, there are no straight forward answers. If the lining is consistently thin, then it is important to assess the inside of the womb cavity with a keyhole camera (hysteroscopy) to see if a reason, for example scar tissues, could be seen. If the lining is thin during a fresh IVF cycle, then the option of freezing all the embryos should be considered. While the embryos are safely in the laboratory, we can try to thicken the womb lining in a frozen cycle, and if we achieve a good endometrial thickness, then we can thaw the embryos and transfer them. In a frozen cycle, high dose oestrogen tablets and patches can be used to thicken the lining. Some clinicians add medicines such as aspirin, steroids, pentoxifylline, tocopherol and Viagra to thicken the endometrium, but there is no clear evidence to support their use. Your IVF consultant would be able to advise the best way forward.
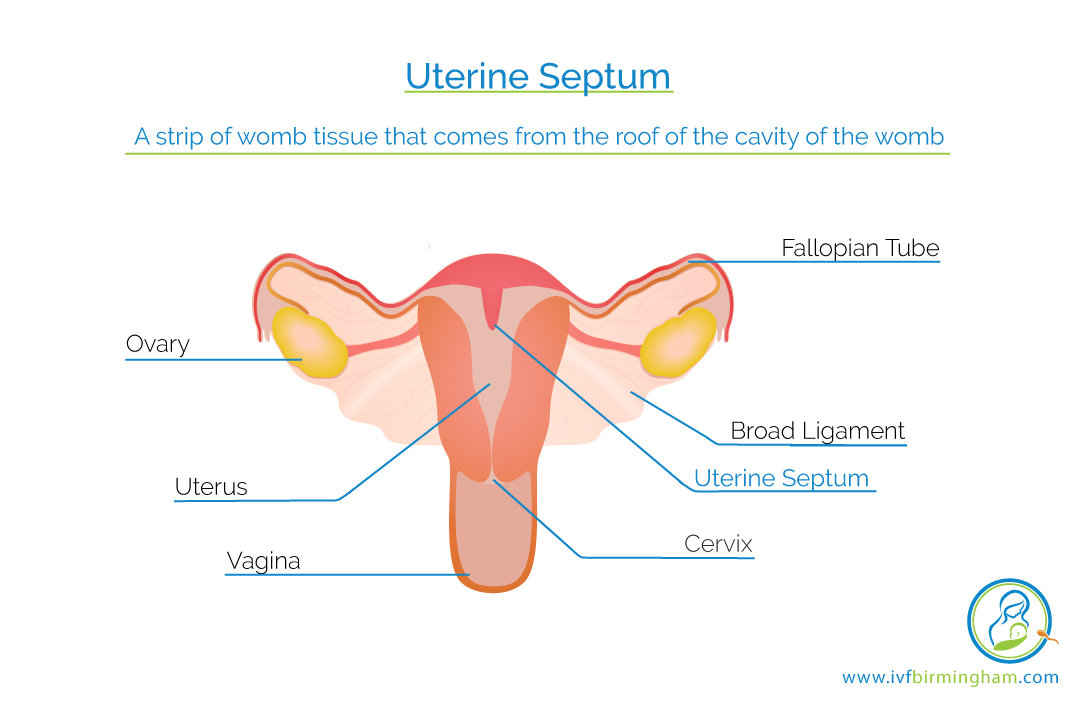
I have been told I have a ‘uterine septum’. What will you advise?
A septum is a strip of womb tissue that comes from the roof of the cavity of the womb, protruding right into the womb cavity. Some septums are very short and do not need any treatment but some may be longer and result in unsuccessful IVF treatment. In these circumstances, your IVF doctor may suggest that you have a camera procedure where the septum can be surgically removed. However, current research is not definite about whether surgery for a septum is of great benefit, and so you should have a good discussion with your doctor before having any surgery.
I have been told I have a ‘uterine septum’. What will you advise?
A septum is a strip of womb tissue that comes from the roof of the cavity of the womb, protruding right into the womb cavity. Some septums are very short and do not need any treatment but some may be longer and result in unsuccessful IVF treatment. In these circumstances, your IVF doctor may suggest that you have a camera procedure where the septum can be surgically removed. However, current research is not definite about whether surgery for a septum is of great benefit, and so you should have a good discussion with your doctor before having any surgery.
How does Covid-19 affect IVF and other fertility treatments?
The British Fertility Society and Association of Reproductive and Clinical Scientists have provided some really useful guidance for patients who have been asking about Covid-19 vaccines and fertility. The availability of safe and effective vaccines against Covid-19 offers a way for many fertility patients to protect themselves against this disease, and access fertility treatment safely.
People of reproductive age should have their covid-19 vaccines when they receive their invitation. This includes all people who are planning fertility treatments now and those who plan for a family in the future.
There is no evidence and no theoretical reason that any of the vaccines can affect the fertility of women or men.
The Covid-19 vaccine can be given during fertility treatment . This includes; IVF, Frozen Embryo Transfer, Egg Freezing, Ovulation Induction, Intra-Uterine Insemination. It may be worth considering to time the Covid-19 vaccine so that you do not have bothersome sides effects, such as fever, headache and muscle aching at the same time as your fertility treatment.
You do not need to delay your fertility treatments until after receiving the vaccines unless you want to be protected from Covid-19 before you become pregnant. Delaying fertility treatments may reduce your chances of pregnancy though.
You can start you fertility treatment immediately after your vaccination. It is also possible to have your Covid-19 vaccine during pregnancy if you are in a risk category for Covid-19. For example, you may be at risk of exposure at work or have an underlying medical condition. If you are not at risk, the current guidance is for the Covid-19 vaccination to be given after pregnancy. There is no evidence that the vaccines are harmful to pregnant women and the available data thus far is reassuring. The vaccine is not a live one and so there is no risk that the vaccine will cause a pregnant woman or her baby to catch Covid-19.
How does Covid-19 affect IVF and other fertility treatments?
The British Fertility Society and Association of Reproductive and Clinical Scientists have provided some really useful guidance for patients who have been asking about Covid-19 vaccines and fertility. The availability of safe and effective vaccines against Covid-19 offers a way for many fertility patients to protect themselves against this disease, and access fertility treatment safely.
People of reproductive age should have their covid-19 vaccines when they receive their invitation. This includes all people who are planning fertility treatments now and those who plan for a family in the future.
There is no evidence and no theoretical reason that any of the vaccines can affect the fertility of women or men.
The Covid-19 vaccine can be given during fertility treatment . This includes; IVF, Frozen Embryo Transfer, Egg Freezing, Ovulation Induction, Intra-Uterine Insemination. It may be worth considering to time the Covid-19 vaccine so that you do not have bothersome sides effects, such as fever, headache and muscle aching at the same time as your fertility treatment.
You do not need to delay your fertility treatments until after receiving the vaccines unless you want to be protected from Covid-19 before you become pregnant. Delaying fertility treatments may reduce your chances of pregnancy though.
You can start you fertility treatment immediately after your vaccination. It is also possible to have your Covid-19 vaccine during pregnancy if you are in a risk category for Covid-19. For example, you may be at risk of exposure at work or have an underlying medical condition. If you are not at risk, the current guidance is for the Covid-19 vaccination to be given after pregnancy. There is no evidence that the vaccines are harmful to pregnant women and the available data thus far is reassuring. The vaccine is not a live one and so there is no risk that the vaccine will cause a pregnant woman or her baby to catch Covid-19.



 treatment")
