We arrange tests at our clinics to investigate for potential reasons for infertility, focusing on the sperm, the eggs and the fallopian tubes. Sometimes we will recommend more advanced tests, called ‘add-on’ tests, to look for complex underlying causes that may be linked to unsuccessful IVF treatment. The tests can be arranged by booking a consultation at our clinics.
We arrange tests at our clinics to investigate for potential reasons for infertility, focusing on the sperm, the eggs and the fallopian tubes. Sometimes we will recommend more advanced tests, called ‘add-on’ tests, to look for complex underlying causes that may be linked to unsuccessful IVF treatment. The tests can be arranged by booking a consultation at our clinics.
If you have been trying to conceive and have not succeeded, you may start to wonder if there is a problem with your eggs, sperm or the fallopian tubes. You may be wondering if you need to have fertility tests. Most clinicians and professional guidelines recommend testing for egg, sperm and fallopian tube problems after 1 year of trying to conceive. What tests should you have? What do the results mean? We provide the answers here. You can book a consultation with us to arrange these tests.
Anti-Mullerian Hormone (AMH) test
AMH test is one of the best tests to assess the store of eggs in your ovaries. It does not tell us exactly how many eggs you have in the ovaries, but it does give a good idea about whether you have a good number of eggs or if your egg count is low in the ovaries. It is a simple blood test, and it can be done at any time in your menstrual cycles (unlike some other hormone tests which need to be done at specific times in your menstrual cycles). The AMH result is usually available after 2 or 3 days after the test. As the AMH result varies by female age, results need to be interpreted in light of the female age and clinical history.
Follicle stimulating hormone (FSH) test
An FSH test can also give an idea about the store of eggs in the ovaries, but it is a less accurate test than AMH. This test needs to done on the 2nd, 3rd, 4th or the 5th day of the menstrual cycle. It is normally combined with Luteinising Hormone (LH) test and sometimes with testosterone hormone measurement to help with the diagnosis of polycystic ovary syndrome. If you have had an AMH test, you would not normally need to have FSH and LH tests.

Follicle stimulating hormone (FSH) test
An FSH test can also give an idea about the store of eggs in the ovaries, but it is a less accurate test than AMH. This test needs to done on the 2nd, 3rd, 4th or the 5th day of the menstrual cycle. It is normally combined with Luteinising Hormone (LH) test and sometimes with testosterone hormone measurement to help with the diagnosis of polycystic ovary syndrome. If you have had an AMH test, you would not normally need to have FSH and LH tests.
Ovulation tests
You can have a urine LH test, progesterone test in the second half of the menstrual cycle, or ultrasound tracking of the follicles (egg sacs in the ovaries) to check if you are releasing eggs from the ovaries. The urine LH test can be purchased from most pharmacies. The progesterone test and the ultrasound follicle tracking are offered at fertility clinics.
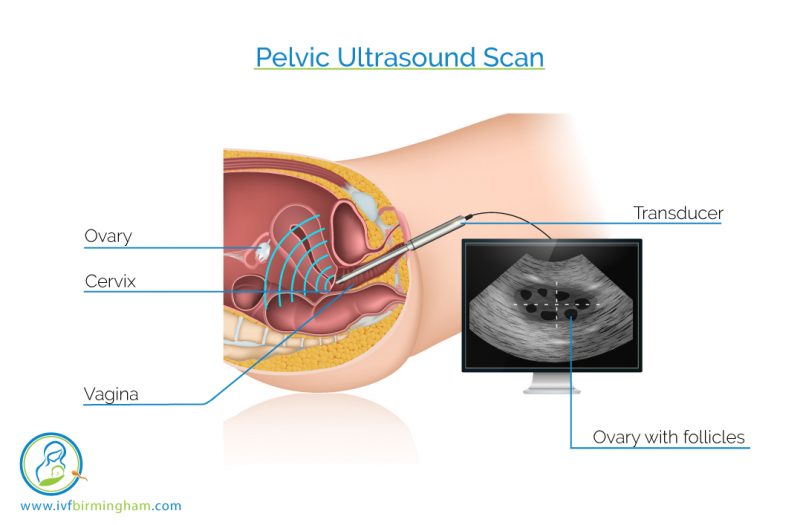
Pelvic Ultrasound Scan
A pelvic ultrasound scan can assess the womb, the ovaries and the fallopian tubes. The assessment of the womb will include looking at the size and position, as well as looking for problems such as fibroids and polyps. The assessment of the ovaries will include looking at the size, nature, location and the number of follicles as well as looking for any cysts. The follicles are small fluid filled sacs that contain the eggs. The follicle count is a good measure of egg count in the ovaries. The ultrasonographer will make a specific assessment of the ovaries to see if they have polycystic appearance or if there is any endometriosis in the ovary. Ultrasound can also help to look for fluid filled blocked fallopian tubes, which are called hydrosalpinges. However, a full assessment of fallopian tubes will need more advanced tests.

Fallopian tube tests
Fallopian tubes can be tested with an X-ray dye test (called hysterosalpingogram) or an ultrasound dye test (called HyCoSy). Both of these tests can be done without the need for anaesthesia. A small plastic tube is passed into the womb and then a dye is injected though this tube. If the fallopian tubes are open, the dye will flow through the fallopian tubes and spill into the pelvic cavity. If a fallopian tube is blocked, then the dye will not flow through it.
Sometimes it may be necessary to do an operation called laparoscopy which involves the surgeon inserting a camera through the belly button to fully assess the fallopian tubes with a dye test. We can also look for endometriosis and even treat endometriosis at laparoscopy.
Semen analysis
Semen analysis involves the careful examination of the semen under a microscope to look at the count (or the concentration), movement (motility) and the shape (morphology) of the sperm. The sperm concentration needs to be more than 15 million per millilitre of semen. Normal sperm motility, or movement, is when at least 40% of sperm are moving. Finally, we want at least 4% of sperm to have normal shape (normal morphology).
The semen needs to be produced by masturbation. There are private rooms in fertility clinics to produce the semen, although some men find it necessary to produce the semen at home and bring it to the clinic for analysis. Whilst this is possible, it is ideal if the semen can be produced in the clinic itself as this will allow us to test a fresh sample. It is important to abstain from ejaculating for 3 days before the sperm test.
Hysteroscopy
A hysteroscopy is a brief operation where a thin telescope camera is inserted through the neck of your womb so that we can see the cavity of the womb. The procedure can be done to check the smoothness and shape of the womb cavity or to help identify and remove polyps (benign growths of the womb lining) or fibroids (benign growths of the muscle of the womb) that may be inside the womb cavity.
Depending on the reason why the hysteroscopy has been advised for you, the procedure can be done whilst you are awake, using a local anaesthetic block to the neck of the womb or with general anaesthetic if required.

There are times when it may be necessary to do a several other tests. These include testing for various hormones such as thyroid hormone levels, checking the chromosomes of the female and male partners, and testing for sticky blood disorders. Occasionally an advanced test such as ERA (Endometrial Receptivity Assay) or immune testing may be suggested. These tests are only needed in very specific circumstances. Moreover, the evidence of benefit is weak for some of the tests; so it is very important to have a full discussion with your fertility doctor before you make up your mind about these tests.The HFEA provides useful information on add-ons in their website
If you wish to discuss these tests, we encourage you to book a consultation with us
Endocrine (hormone) tests
Your doctor may advise you have tests for various hormones, including thyroid function, prolactin, male hormone levels and tests for diabetes. These tests are not needed for everyone; they are only if the doctor suspects you are at risk of an endocrine (hormone) problem. So, don’t worry if you are not offered these tests by the fertility specialist.
Some hormonal imbalances are relatively straightforward to treat. An example is underactive thyroid where the reduced function of the thyroid gland may be compensated by giving thyroxine tablets.
If the condition involves overproduction of a particular hormone, like in hyperprolactinemia or hyperthyroidism, the treatment involves administering medication to reduce the production of these hormones.
In other instances we need to incorporate lifestyle changes to improve the reproductive outcome, and involve endocrine specialists to help manage conditions such as diabetes.
Chromosome (karyotype) tests
Genes are the blueprints that determine how every part of each of our bodies develops and functions. Our genes are organised into 23 pairs (that is 46 in total) of chromosomes which are present inside every cell in our body. One of each of the pairs comes from each of our parents.
Some people have unusual arrangements of these chromosomes which are called chromosomal translocations. If either of the couple has a chromosomal translocation, then they are at high risk of having repeated pregnancy losses. So, if you have had a large number of pregnancy losses, the doctors may want you to have a blood test to check for your chromosomes. If you are found to have a chromosome problem, you will be seen by a genetics specialist, and you may be recommended to have an advanced form of IVF called PGD (Pre-implantation Genetic Diagnosis).

Chromosome (karyotype) tests
Genes are the blueprints that determine how every part of each of our bodies develops and functions. Our genes are organised into 23 pairs (that is 46 in total) of chromosomes which are present inside every cell in our body. One of each of the pairs comes from each of our parents.
Some people have unusual arrangements of these chromosomes which are called chromosomal translocations. If either of the couple has a chromosomal translocation, then they are at high risk of having repeated pregnancy losses. So, if you have had a large number of pregnancy losses, the doctors may want you to have a blood test to check for your chromosomes. If you are found to have a chromosome problem, you will be seen by a genetics specialist, and you may be recommended to have an advanced form of IVF called PGD (Pre-implantation Genetic Diagnosis).
Immune or Natural Killer Cell testing
Couples who have had repeated unsuccessful IVF attempts or recurrent miscarriages often wonder if their bodies’ own immunity may be ‘rejecting’ the pregnancy. A lot of women particularly worry about having high levels of Natural Killer Cells.
Natural killer, or for short NK, cells are a type of white blood cells that fight infection and cancer cells. The natural killer cells also play an important role in implantation, the process by which an embryo takes hold in the lining of the womb. But we don’t yet fully understand exactly how they help or hinder implantation.
Researchers have conducted many studies to find out how NK cells are linked to repeated unsuccessful IVF cycles or recurrent miscarriages. Unfortunately, the evidence is not clear cut. So, for example, if you look at studies that looked at blood NK cells, 8 studies found that NK cells were increased in women with recurrent miscarriages, but in contrast, 3 studies found that there was no difference in NK cell levels between patients who had recurrent miscarriages and control patients without miscarriages. So, although the weight of evidence suggests a higher level of NK cells in those with repeated IVF failures or recurrent miscarriages, uncertainties remain.
How do we test for NK cells? We can check for the NK cells in the blood, or in the womb. Testing in the womb will need a biopsy. If the NK cell levels are high, then your doctor may discuss treatment with you. It is really important that you and your doctor have a frank and open discussion about the limited evidence and the huge uncertainties around both NK cell testing and immune therapy. You should also carefully consider the potential adverse effects. After careful consideration, if immune therapy is considered a reasonable step, the potential treatment options include: progesterone, heparin, prednisolone and intralipid.
Scientific Research Summary
Immune or Natural Killer Cell testing
Couples who have had repeated unsuccessful IVF attempts or recurrent miscarriages often wonder if their bodies’ own immunity may be ‘rejecting’ the pregnancy. A lot of women particularly worry about having high levels of Natural Killer Cells.
Natural killer, or for short NK, cells are a type of white blood cells that fight infection and cancer cells. The natural killer cells also play an important role in implantation, the process by which an embryo takes hold in the lining of the womb. But we don’t yet fully understand exactly how they help or hinder implantation.
Researchers have conducted many studies to find out how NK cells are linked to repeated unsuccessful IVF cycles or recurrent miscarriages. Unfortunately, the evidence is not clear cut. So, for example, if you look at studies that looked at blood NK cells, 8 studies found that NK cells were increased in women with recurrent miscarriages, but in contrast, 3 studies found that there was no difference in NK cell levels between patients who had recurrent miscarriages and control patients without miscarriages. So, although the weight of evidence suggests a higher level of NK cells in those with repeated IVF failures or recurrent miscarriages, uncertainties remain.
How do we test for NK cells? We can check for the NK cells in the blood, or in the womb. Testing in the womb will need a biopsy. If the NK cell levels are high, then your doctor may discuss treatment with you. It is really important that you and your doctor have a frank and open discussion about the limited evidence and the huge uncertainties around both NK cell testing and immune therapy. You should also carefully consider the potential adverse effects. After careful consideration, if immune therapy is considered a reasonable step, the potential treatment options include: progesterone, heparin, prednisolone and intralipid.
Scientific Research Summary
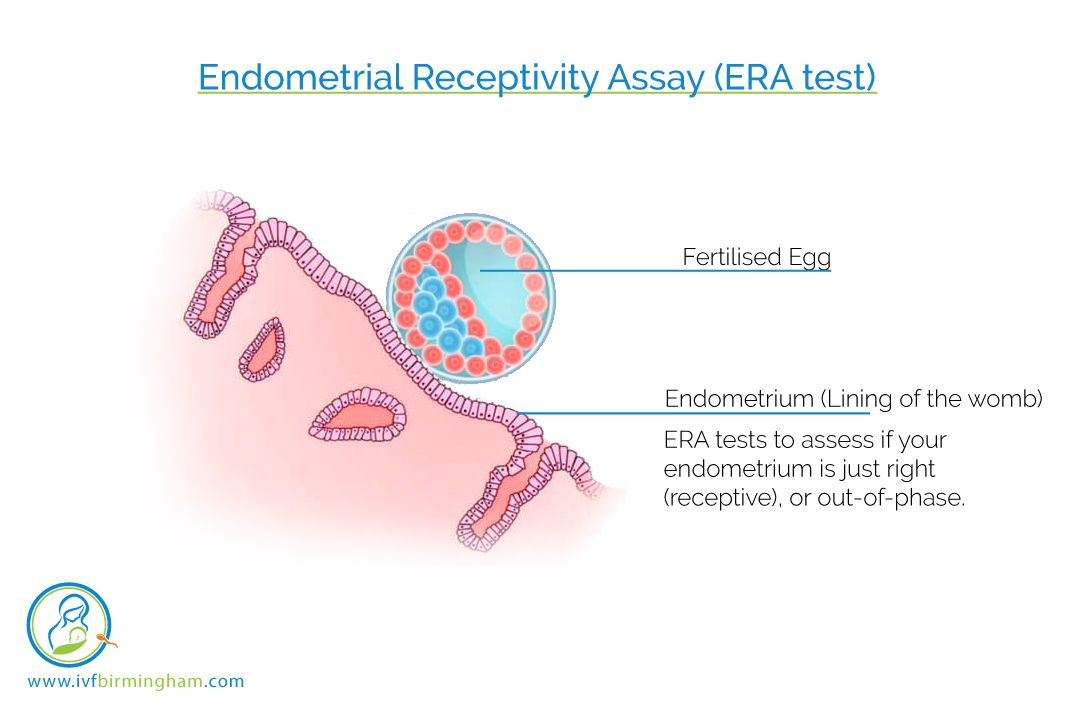
Endometrial Receptivity Assay (ERA test)
If you have had repeated unsuccessful IVF cycles despite transfer of good quality embryos, a natural question is whether there is a problem in the lining of the womb (endometrium). The ERA test is designed to assess if your endometrium is just right (receptive), or out-of-phase to help with implantation of the embryo. It is a molecular diagnostic test based on microarray technology looking at the expression of 248 selected genes. The test is done on a biopsy taken from the lining of the womb. Following the test, women then undergo personalized embryo transfer (pET) where the frozen–thawed embryo transfer is timed according to the receptive status as identified by ERA.
Five studies reported clinical outcomes following the use of ERA and pET in women with previous unsuccessful embryo transfers. These studies were not ‘randomised control trials’, meaning the evidence from them cannot be regarded high quality and free of biases. Nevertheless, they all suggested benefit, so it may be reasonable for you to discuss the potential role of this test with your fertility doctor.
Scientific Research Summary
Thrombophilia (‘Sticky blood disorders’) tests
Thrombophilias are a collection of blood disorders in which the patient has an increased tendency for blood clots developing in blood vessels. If you have thrombophilia, you have an imbalance in the clotting chemicals and proteins in your blood which puts you at an increased risk of a blood clot. That is why thrombophilias are called “sticky blood disorders”.
Thrombophilias can be of two types: inherited or acquired. Inherited thrombophilias are those which are dependent on the genes you inherited from you parents. They include factor V Leiden, prothrombin gene mutation and protein C, protein S and anti-thrombin deficiency. You may have family members who are also affected. Acquired thrombophilias are those acquired during your lifetime, that is, you were not born with them, but developed them at some time in the past. The key disorder here is antiphospholipid syndrome.
We know that both inherited and acquired thrombophilias bring an increased risk of complications in pregnancy. The complications include miscarriage, growth restricted babies, pre-eclampsia and stillbirth. These complications appear to be the result of two processes: one is thrombosis, in which blood clots develop in the narrow blood vessels of the placenta and the lining of the womb. And the other is inflammation that triggers an immune response.
Specialised blood tests can be done to look for thrombophilia. If you have a sticky blood disorder, treatment will involve blood thinning drugs. The drugs are aspirin and low molecular weight heparin. You may be given clexane or fragmin, two common low molecular weight heparin preparations.
Sperm DNA fragmentation test
Good quality sperm DNA is important for achieving fertility and avoiding miscarriages. Sperm DNA normally has some breaks (or fragmentation) but if the level of fragmentation is high, this can affect pregnancy chances. So, it may sometimes be helpful to test the DNA of the sperm, particularly when the couples have suffered repeated unsuccessful IVF attempts or recurrent miscarriages. We can test for sperm DNA damage using semen produced by masturbation. Studies from our research group have shown that women with partners who have high levels of sperm DNA damage are 4 times more likely to miscarry compared with women with partners who have low levels of sperm DNA damage.
If there are high levels of sperm DNA fragmentation, the first step is to address lifestyle choices that are damaging your sperm’s DNA. These include smoking, alcohol, recreational drugs and poor diet, particularly consumption of processed meat. Your doctor may also discuss with you the use of ICSI treatment or use of testicular sperm for ICSI treatment.
If you would like to know more about any of these tests, do book a consultation with one of our specialist fertility doctors.
Scientific Research Summary
